Real-World Cases Illustrate Our Cutting-Edge Techniques
At Main Street Radiology, we offer a combination of advanced technology and professional expertise. Our doctors and radiologists have a long record of success in using sophisticated equipment, software and techniques to better serve our patients. These case studies illustrate how our resources come together to provide state-of-the-art medical tests and treatments.
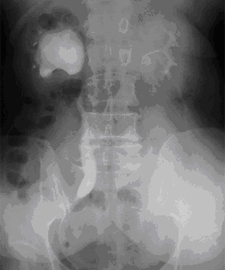
Figure 1
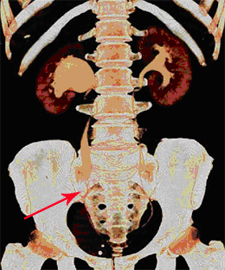
Figure 2
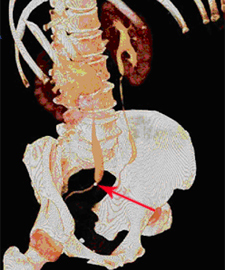
Figure 3
History: 61-year-old male with hematuria. IVP was performed (Figure 1) demonstrating severe dilatation of the right collecting system and dilatation of the mid ureter, of uncertain etiology. The patient was referred to Main Street Radiology for a CT scan of the abdomen and pelvis.
Findings: As part of "hematuria protocol" CT, 3D CT urography was performed (Figures 2-3). A distal right ureteral calculus is seen (arrow) resulting in dilatation of the mid right ureter. Right UPJ obstruction is also note
Discussion: With a 16-detector spiral CT, 3D volumetric imaging can be obtained. There are numerous applications which have revolutionized medical imaging. In studying the urinary tract, 3D images surpass the diagnostic capabilities of IVP and routine CT.
At MSR, "hematuria protocol" CT routinely involve acquisition of 3D CT urography images, as well as the traditional pre- and post-contrast thin section axial images of the kidneys.
MSR is the first facility in Queens with a 16-detector spiral CT and one of the few centers in the New York area to routinely perform CT urography.
Case History: 52-year-old asymptomatic male smoker with mildly elevated cholesterol and family history of coronary artery disease, volunteered for CT coronary angiography at Main Street Radiology.
Technique: Oral beta-blocker was administered the night prior to the exam to reduce the heart rate below 70 bpm. 100 cc of intravenous contrast was administered during a 20 second breath-hold. EKG-gated images were obtained on a 16-detector spiral CT.
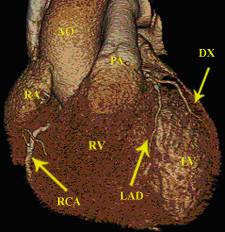
Figure 1
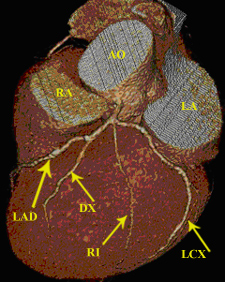
Figure 2
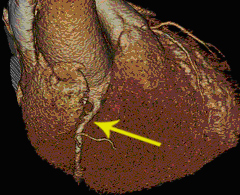
Figure 3
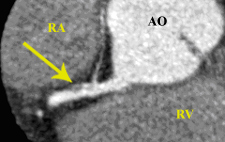
Figure 4
Findings: 3D anterior image of heart (figure 1) outlines normal anatomy (AO = aorta; PA = pulmonary artery; RA = right atrium; RCA = right coronary artery; LAD = left anterior descending artery; RV = right ventricle; LV = left ventricle; DX = diagonal branch). 3D oblique image of the left coronary arteries (figure 2) demonstrates no significant stenosis (LCX = left circumflex artery; RI = ramus intermedius). 3D oblique image of the RCA demonstrates focal stenosis proximally (arrow). A non-calcified (soft) plaque (arrow) is seen on the 2D axial-oblique image of the right coronary artery (figure 4), with approximately 40% stenosis.
Recommendations: Aggressive intervention to reduce risk factors.
Discussion: In October 2003, MSR installed the first 16-detector spiral CT in Queens. With this new technology, we are one of the first facilities in the New York area to perform many sophisticated studies including CT coronary angiography.
The 16-detector CT enables "isotropic" volume acquisition, where true 3D images can be obtained in every projection. Previously available CT technology suffered from loss in resolution when images were viewed at different angles. Coronary arteries can now be viewed at the highest resolution, not dependent on its orientation. In addition, due to its unprecedented speed, the 16 detector CT can effectively "freeze" cardiac motion for heart rates less than 70 bpm.
Early reports indicate that CT coronary angiography may ultimately replace diagnostic cardiac catheterization, with reported sensitivity of 95% (Nieman, Circulation 2002; 106 (16): 2051-4).
Advantages of CT coronary angiography include:
- CT angiography is non-invasive, only requiring IV injection of iodinated contrast
- Less expensive
- Aside from the lumen, the vessel wall and plaque can be imaged and characterized ("soft" vs. "hard" plaque)
- 2D and 3D images can be viewed at every angle and in cross section, increasing accuracy of grading of stenosis
As up to 50% of diagnostic cardiac catheterizations fail to show significant disease, CT coronary angiography may take on an important role in screening patients with indications for cardiac catheterization. As more studies are published in the medical literature, indications for CT coronary angiography should be better defined.
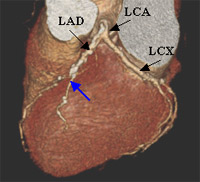
Figure 1
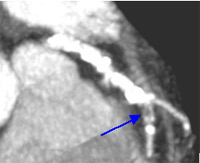
Figure 2
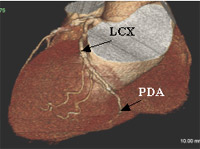
Figure 3

Figure 4
Case History: 67-year-old male with history of hypertension and elevated cholesterol presented with atypical chest pain. Nuclear medicine cardiac stress test was negative. The patient was referred to Main Street Radiology for CT coronary angiography.
Findings: 3D image of the heart (figure 1) shows atherosclerotic changes of the left main (LCA), left anterior descending (LAD) and left circumflex (LCX) arteries, manifested by irregular contour of the vessels. Focal stenosis of the LAD is seen (blue arrow) near the origin of the first diagonal branch. This finding is confirmed on the 2D image (figure 2) where "soft" (non-calcified) plaque (arrow) results in approximately 70% stenosis. Additional 3D images (figures 3 and 4) show a left dominant system, manifested by prominent LCX supplying the posterior descending artery (PDA) and small right coronary artery (RCA).: 3D image of the heart (figure 1) shows atherosclerotic changes of the left main (LCA), left anterior descending (LAD) and left circumflex (LCX) arteries, manifested by irregular contour of the vessels. Focal stenosis of the LAD is seen (blue arrow) near the origin of the first diagonal branch. This finding is confirmed on the 2D image (figure 2) where "soft" (non-calcified) plaque (arrow) results in approximately 70% stenosis. Additional 3D images (figures 3 and 4) show a left dominant system, manifested by prominent LCX supplying the posterior descending artery (PDA) and small right coronary artery (RCA).
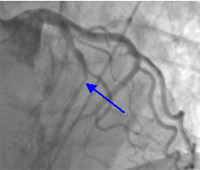
Figure 5
Conventional angiogram was performed which confirmed the presence of significant LAD stenosis (arrow on figure 5). Angioplasty and stenting was subsequently performed with satisfactory results.
Discussion: In November 2003, Main Street Radiology performed the first CT coronary angiography in Queens.
Early reports indicate that CT coronary angiography may ultimately replace diagnostic cardiac catherization, with reported sensitivity of 95% (Nieman, Circulation 2002; 106 (16): 2051-4). This is significantly higher than the sensitivity of nuclear medicine stress test, reported in the range of 80-85%.
The main advantage of CT coronary angiography over cardiac catherization, is that it is non-invasive, only requiring IV injection of iodinated contrast. In addition, the nature of the plaque, whether soft or hard, can be assessed with CT coronary angiography. In the past, only endovascular ultrasound was able to differentiate soft or "vulnerable" plaque.
Medicare announced in 2004 that CT coronary angiography will be reimbursed in Queens. This decision was based on reports showing "high correlation with stenotic lesions noted on diagnostic cardiac catherization, but more importantly, with atheromas on intracoronary ultrasound."